
burn wound depth
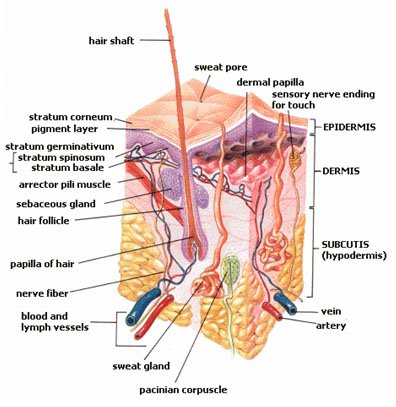
Diagram of the skin - composed of the superficial epidermis, underlying dermis and deeper subcutaneous tissues
Source: Wikipedia
Classification of burn wound depth
The first classification, proposed by Fabry related to three degrees of ‘intensity’ of burn;
- redness and blistering of skin
- withering of skin (without charring)
- eschar formation and charring
From this, a further classification system developed – with only two degrees of severity: (Jackson 1953)
- partial thickness skin loss – implying sufficient living epithelial elements present to resurface the area
- full thickness skin loss – implying virtually complete destruction of all epithelial elements, with healing carried out by the contraction of wound edges.
The definitive diagnosis is based on the histological depth of tissue necrosis (from a punch biopsy of the skin), but this is an invasive procedure, and other techniques have been utilised such as the use of laser Doppler to assess blood flow dynamics and flow motion patterns and hence infer the likely wound healing outcome, in place of clinical depth assessment (McClance and Huether 2002 p.1499, Yeong et al 1996 pp.956-961). Devgan et al (2006) have recently reviewed methods for estimation of burn wound depth, in an 'open access' article.
The classification systems can be combined to provide the following subdivisions;
- first degree
- second degree
- superficial partial thickness
- deep partial thickness
- third degree - full-thickness

Degrees of burns
Source: Wikipedia
first degree burns

Sunburn (2 days following 5 hour exposure)
Source: Wikipedia
These wounds involve the epidermis (e.g. as seen in ‘sunburn’), and are characterised by local pain and erythema, with blister formation after approximately 24 hours. When severe, there can be systemic symptoms associated with the burn, including headache, nausea and vomiting and chills. The young and elderly in particular may require rehydration and analgesia, if severe.
second degree burns

Burn caused by direct contact with hot oven - within minutes
Source: Wikipedia

Evolution of same burn - after 1 day
Source: Wikipedia

Evolution of same burn - after 2 days
Source: Wikipedia
Superficial partial thickness
These wounds are characterised by blistering (thin walled and fluid filled) and extreme pain. This is because nerve endings are exposed throughout the healing process and cause pain for approximately 3-4 weeks. Tissue regeneration takes place from proliferation of epithelial cells from hair follicles and sweat gland ducts. Scar formation is minimal. The tissue under the blister is moist, pink and blanching.
Deep partial thickness
These burn wounds affect the dermis to a variable depth. The involvement of skin appendages, such as hair follicles etc is also variable, but they are more involved than superficial wounds and therefore the rate of healing is slower. The wounds appear pink to white with blistering. They tend to be dry and hypo-aesthetic, being surrounded by superficial burn wounding. During the healing process, residual undamaged skin appendages give rise to skin buds and hair follicles. In view of the increased healing time associated with these wounds, they are invariably excised and replaced by grafts, to reduce the scar burden.
third degree burns
These wounds extend to variable depths of the subcutaneous tissue, and can involve muscle and bone (sometimes referred to as 4th degree burn wounds).
The wounds are dry and leathery, and there are often thrombosed subcutaneous vascular plexi visible. They are hypoaesthetic, as all sensory nerves have been destroyed.
The colour of these wounds varies – from white or black (charring), to red or cherry red (effect of carbon monoxide uptake in the tissues). The colour does not blanch. As oedema develops, distal circulation may be compromised (particularly in circumferential limb burns) and escharotomies are performed.
The depth of burn is not static, however, and wounds can evolve over time (becoming deeper if not adequately managed) (McClance and Huether 2002 pp.1499-1501, Barret and Herndon 2001 pp.2-7 and Wardrope 1992 pp. 189-191).

Third degree burns
Source: Wikimedia Commons

Third degree burns
Source: Pflegewiki

Third degree burns
Source: Wikipedia
references
- Barret J.P., Herndon D.N. (Ed)(2001), ‘Colour Atlas of Burn Care’, W.B. Saunders
- Devgan L, Satyanarayan B, Aylward BA, Spence RJ (2006), 'Modalities for the assessment of burn wound depth', Journal of Burns and Wounds 5:e2 (published online 18/2/2006) (https://www.pubmedcentral.nih.gov/picrender.fcgi?artid=1687143&blobtype=pdf)
- Jackson D.M. (1953), ‘The diagnosis of the depth of burning’, British Journal of Surgery 40:588-596
- McClance K.L., Huether S.E. (2002), ‘Pathophysiology. The biologic basis for disease in adults and children’, 4th Ed Mosby Inc.
- Wardrope J., Smith J.A.R. (1992), ‘The management of Wounds and Burns’, Oxford University Press
- Yeong E.K., Mann R., Goldberg M., Engrav L., Hembach D. (1996), ‘Improved accuracy of burn wound assessment using laser doppler’, Journal of Trauma 40(6):956-961